|
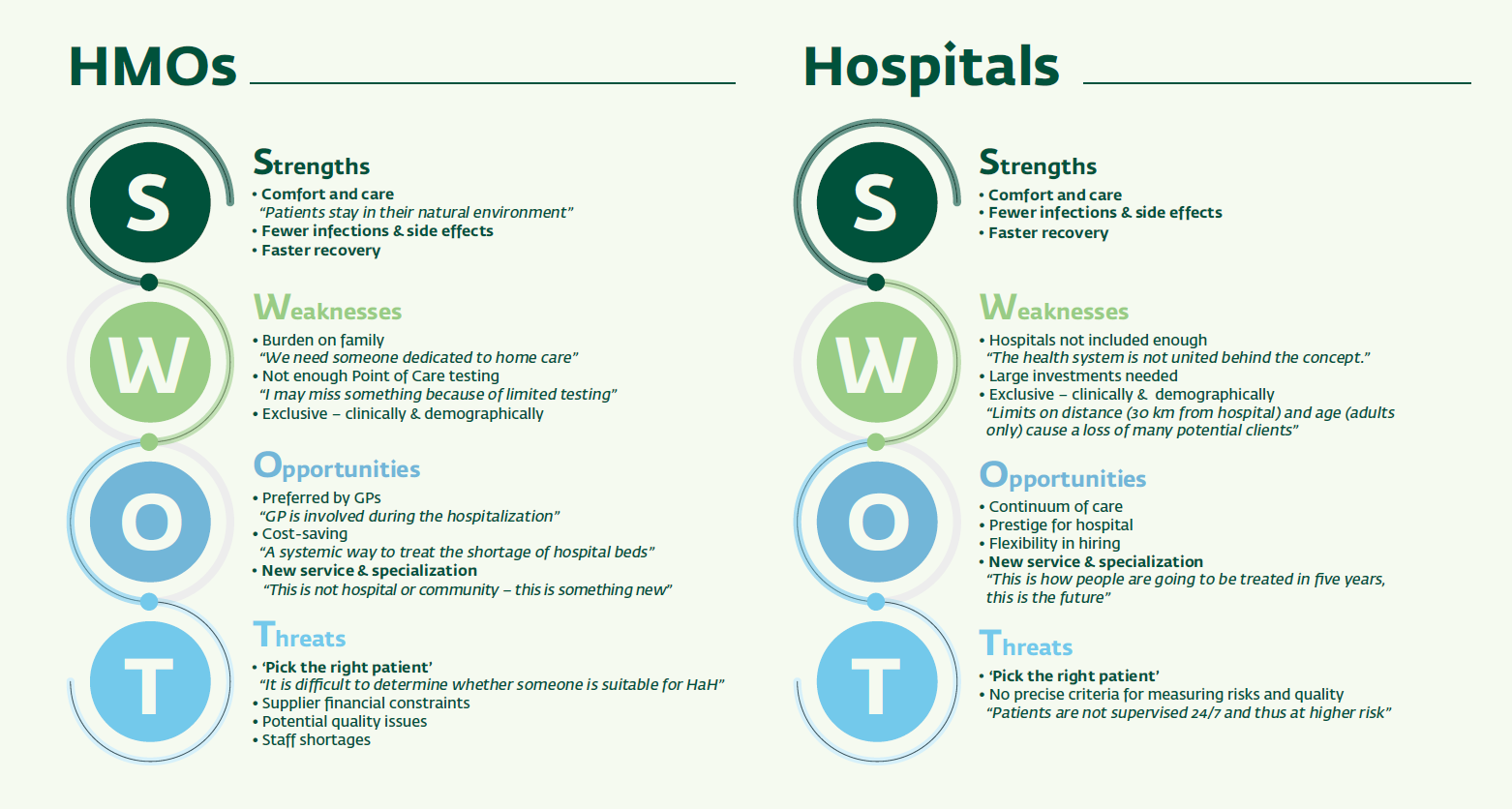
HOSPITAL AT HOME - Who should provide it? A SWOT analysis of managers' attitudes to HOSPITAL AT HOME


In reply to First post
Re: HOSPITAL AT HOME - Who should provide it? A SWOT analysis of managers' attitudes to HOSPITAL AT HOME
by WHAHC Community Team -
Log in and add your comments or questions for Neta Harel and Prof. Racheli Magnezi to answer here.